[Reblog] A 5-star rating system for nursing homes and the unintended consequences on health care disparities
From the 8 May 2015 post at Science Health
Information about the quality and performance of health care facilities can be confusing to consumers. Dozens of government organizations, trade groups and websites rate doctors, hospitals and long-term care facilities on all kinds of scales, from patient satisfaction to medical outcomes.
In 2008, the Centers for Medicare and Medicaid Services (CMS) attempted to simplify some of this data by creating a five-star rating system for nursing homes. The idea was that public reporting would drive improvement in care, helping nursing home residents and their families choose higher quality facilities, in turn encouraging nursing homes to improve quality to retain residents.
This data can be of limited use, however, for people whose decisions are constrained by insurance networks, cost and geography. People who are enrolled in both Medicare and Medicaid, often called “dual eligibles,” are particularly limited in their choices for long-term care. They are much more likely to have lower incomes, disabilities or cognitive impairment, and to receive low-quality health care in poor neighborhoods than other Medicare beneficiaries.
A new study in the May issue of Health Affairs by public health researchers from the University of Chicago, Harvard, and Penn confirms that despite best intentions, the new rating system exacerbated health disparities between this dual eligible group and non-dual eligible nursing home residents, i.e. those with better financial support. By 2010, two years after the system began, both groups lived in higher quality nursing homes overall, but non-dual eligible residents were more likely to actively choose a higher-rated nursing home. The gap between the two groups also increased: dual eligibles were still more likely to live in a one-star home, and less likely than non-dual eligibles to live in a top-rated home.
…

[News release] Insuring undocumented residents could help solve multiple U.S. health care challenges
From the 18 March 2015 UCLA news release
UCLA health care policy analysis finds four key problem areas for Latinos under Affordable Care Act
Latinos are the largest ethnic minority group in the United States, and it’s expected that by 2050 they will comprise almost 30 percent of the U.S. population. Yet they are also the most underserved by health care and health insurance providers.
Latinos’ low rates of insurance coverage and poor access to health care strongly suggest a need for better outreach by health care providers and an improvement in insurance coverage. Although the implementation of the Affordable Care Act of 2010 seems to have helped (approximately 25 percent of those eligible for coverage under the ACA are Latino), public health experts expect that, even with the ACA, Latinos will continue to have problems accessing high-quality health care.
Alex Ortega, a professor of public health at the UCLA Fielding School of Public Health, and colleagues conducted an extensive review of published scientific research on Latino health care. Their analysis, published in the March issue of the Annual Review of Public Health, identifies four problem areas related to health care delivery to Latinos under ACA:
- The consequences of not covering undocumented residents.
- The growth of the Latino population in states that are not participating in the ACA’s Medicaid expansion program.
- The heavier demand on public and private health care systems serving newly insured Latinos.
- The need to increase the number of Latino physicians and non-physician health care providers to address language and cultural barriers.
“As the Latino population continues to grow, it should be a national health policy priority to improve their access to care and determine the best way to deliver high-quality care to this population at the local, state and national levels,” Ortega said. “Resolving these four key issues would be an important first step.”
Insurance for the undocumented
Whether and how to provide insurance for undocumented residents is, at best, a complicated decision, said Ortega, who is also the director of the UCLA Center for Population Health and Health Disparities.
For one thing, the ACA explicitly excludes the estimated 12 million undocumented people in the U.S. from benefiting from either the state insurance exchanges established by the ACA or the ACA’s expansion of Medicaid. That rule could create a number of problems for local health care and public health systems.
For example, federal law dictates that anyone can receive treatment at emergency rooms regardless of their citizenship status, so the ACA’s exclusion of undocumented immigrants has discouraged them from using primary care providers and instead driven them to visit emergency departments. This is more costly for users and taxpayers, and it results in higher premiums for those who are insured.
In addition, previous research has shown that undocumented people often delay seeking care for medical problems.
…
As the ACA is implemented and more people become insured for the first time, local community clinics will be critical for delivering primary care to those who remain uninsured.
“These services may become increasingly politically tenuous as undocumented populations account for higher proportions of clinic users over time,” he said. “So it remains unclear how these clinics will continue to provide care for them.”
..
[Reblog] Going Viral: The Re-Emergence of Preventable Diseases
From the 19 February 2015 post at Policy Interns
From an aging population to the growing threat of pandemic influenza and other emerging infectious diseases as well as the rapid growth of obesity and other chronic illnesses, the most persistent and costly challenges to American health and well-being fall increasingly on the public health system and on public health professionals at all levels. Unlike health care, which often intervenes when an individual is already sick with a costly disease, the focus of public health is prevention rather than treatment of diseases. Public health professionals, working with state and local health departments, laboratories, and other public health organizations, play a vital and increasingly central role in protecting a population’s health. Yet the Center for Disease Control (CDC) and other public health observers have repeatedly identified deficiencies in public health infrastructure and workforce.
Regional interstate planning, preparing for mass vaccination and the distribution of medical supplies, and development of adequate surge capacity are incomplete or insufficient. The Government Accountability Office concluded in 2004 that “no State is fully prepared to respond to a major public health threat,” an assessment that the CDC reiterated in 2008.
One might look at Figure 1 and think, where are the lines for public health expenditures on federal, state, and local levels? They’re there, almost completely parallel to the x-axis. Federal public health spending underperformed a number of other U.S. health sector expenditure categories overall. As a percentage of all U.S. health expenditures, federal public health spending was lower in 2008 than it was in 1966. To make matters worse, the Fiscal Year 2015 request proposes a $51 million decrease for the immunization program due to an expectation of increased insurance coverage for immunization services in 2015. This is yet another cut to public health spending that will undoubtedly affect population health.
Program operations, which contribute to disease surveillance, public awareness and provider education, took a $14 million cut.
…
While proponents of the ACA said the majority of the proposed fiscal 2016 cuts again will go toward vaccine purchasing and won’t affect immunization infrastructure funds, this cannot be the whole picture. The families and children currently using these programs will be in jeopardy because insurance coverage alone is not enough to ensure high vaccination rates.
…

Related articles







[Reblog] A ‘birth lottery’ still determines who gets to live longest, healthiest life
A ‘birth lottery’ still determines who gets to live longest, healthiest life | joe rojas-burke.
From the 16 June 2014 post at JOE ROJAS-BURKE- Science Writer
…
The latest data suggest that lack of social mobility remains as significant a problem as it was decades ago. In the generation entering the U.S. workforce today, those who started life in the bottom fifth of income distribution have about a 9 percent chance of reaching the top fifth. That compares with an 8.4 percent chance for kids born in 1971, according to research by economists Raj Chetty of Harvard, Emmanuel Saez of the University of California, Berkeley, and colleagues.
What’s astonishing are the huge differences in mobility depending on where you grow up, The odds of escaping poverty and gaining prosperity are less than 3 percent for kids in many places across the South and Rust Belt states. But in some parts of the Great Plains, more than 25 percent of kids born to the poorest parents move into the upper-income strata as adults, the economists found. The datasets are available here.
I don’t think it’s a coincidence that the places on this map with the lowest social mobility also tend to have the worst health outcomes. Lack of mobility is strongly correlated with worse segregation, greater income inequality, poor local school quality, diminished social capital, and broken family structure – factors that are also linked to poor health.
Even when poor children manage to escape poverty, a “birth lottery” may still determine who gets to live longest and healthiest. Exposure to adverse conditions during fetal development and early infancy appears to be capable of causing irreversible consequences decades later, such as increased vulnerability to weight gain, diabetes, heart disease, and premature death.
…

Related articles


[Press release] Zip code better predictor of health than genetic code
Zip code better predictor of health than genetic code | HSPH News | Harvard School of Public Health.
From the 4 August 2014 Harvard School of Public Health News item
In St. Louis, Missouri, Delmar Boulevard marks a sharp dividing line between the poor, predominately African American neighborhood to the north and a more affluent, largely white neighborhood to the south. Education and health also follow the “Delmar Divide,” with residents to the north less likely to have a bachelor’s degree and more likely to have heart disease or cancer.
Pointing to Delmar as an example, Melody Goodman, an assistant professor at Washington University in St. Louis, recently spoke to a Harvard School of Public Health (HSPH) audience about the links between segregation and poor health. An HSPH alumna, Goodman gave the keynote address at the first annual symposium sponsored by the Department of Biostatistics Summer Program in Quantitative Sciences. She told the audience at the July 24, 2014 event, which was held at Dana-Farber Cancer Institute, “Your zip code is a better predictor of your health than your genetic code.”
Related articles


[News article] Dental care in school breaks down social inequalities
From the 10 February 2014 Science Daily article
A new global survey documents how dental care in the school environment is helping to assure a healthy life and social equity — even in developing countries. But there are still major challenges to overcome worldwide.
…
Around 60 per cent of the countries that took part in the study run formalized teaching in how to brush teeth, but not all countries have access to clean water and the necessary sanitary conditions. This constitutes a major challenge for the health and school authorities in Asia, Latin America and Africa in particular.
English: ADA/Dental Health on US postage stamp (Photo credit: Wikipedia)
“Countries in these regions are battling problems involving the sale of sugary drinks and sweets in the school playgrounds. Selling sweets is often a source of extra income for school teachers, who are poorly paid,” explains Poul Erik Petersen.
He continues: “This naturally has an adverse effect on the children’s teeth. Many children suffer from toothache and general discomfort and these children may not get the full benefit of their education.”
The biggest challenges to improved dental health in low-income countries are a lack of financial resources and trained staff. Schools in the poorest countries therefore devote little or no time to dental care, and they similarly make only very limited use of fluoride in their preventative work. Moreover, the healthy schools in low-income countries find it harder to share their experience and results.
Social inequality is a serious problem
Social inequality in dental health and care is a serious problem all over the world:
“However, inequality is greater in developing countries where people are battling with limited resources, an increasing number of children with toothache, children suffering from HIV/AIDS and infectious diseases — combined with a lack of preventive measures and trained healthcare staff,” says Poul Erik Petersen, before adding:
“Even in a rich country like Denmark, we see social inequalities to dental care, despite the fact that dental health here is much improved among both children and adults. The socially and financially disadvantaged groups of the population show a high incidence of tooth and mouth complaints compared with the more affluent groups.”
…


[Press Release] Greatest economic burden shouldered by African-American and Hispanic men
From the 22 January 2014 press release
Greatest economic burden shouldered by African-American and Hispanic men
African-American men incurred $341.8 billion in excess medical costs due to health inequalities between 2006 and 2009, and Hispanic men incurred an additional $115 billion over the four-year period, according to a new study by researchers at the Johns Hopkins Bloomberg School of Public Health. The study, published this week in the International Journal of Men’s Health, looks at the direct and indirect costs associated with health inequalities and projects the potential cost savings of eliminating these disparities for minority men in the U.S.
“Health disparities have a devastating impact on individuals and families, and they also affect society as a whole,” said Roland J. Thorpe, Jr., PhD, lead author of the study and Assistant Professor at the Johns Hopkins Bloomberg School of Public Health and Director of the Program for Research on Men’s Health in the Johns Hopkins Center for Health Disparities Solutions. “Quantifying the economic impact of health inequalities among men highlights how enormous a societal problem this is.”
Researchers used data from the Agency for Health Care Research and Quality’s 2006-2009 Medical Expenditure Panel Survey (MEPS) to determine the prevalence of a variety of health statuses and conditions (for example, fair/poor health, obesity, diabetes, heart disease) among each racial/ethnic group (African American, Asian, Hispanic and white). This information was incorporated in statistical models to estimate the total direct medical costs and the proportion of costs incurred due to health disparities for each group. The direct medical expenditures for African-American men over the four-year period totaled $447.6 billion; and 5.4 percent, or $24.2 billion, were excess costs attributed to health disparities. There were no excess direct costs due to health disparities for the other racial/ethnic groups over the four year period.
The indirect costs of lower worker productivity due to illness and premature death were calculated using data from MEPS and the CDC’s National Vital Statistics System. Over the four-year period, these factors cost the economy a total of $436.3 billion—lower worker productivity due to illness contributed $28 billion in excess costs, and premature death contributed $408.3 billion. Of the total indirect costs, African-American men accounted for $317.6 billion, or 72 percent; indirect costs totaled $115 billion for Hispanic men and $3.6 billion for Asian men.
“These stark findings underscore the fact that we can’t afford to overlook men’s health disparities that exist in this country,” added Thorpe. “The cost to society—both moral and economic—is staggering.”
Related articles





[Press release] Health disparities among US African-American and Hispanic men cost economy more than $450 billion
From the 22 January 2014 press release
Greatest economic burden shouldered by African-American and Hispanic men
African-American men incurred $341.8 billion in excess medical costs due to health inequalities between 2006 and 2009, and Hispanic men incurred an additional $115 billion over the four-year period, according to a new study by researchers at the Johns Hopkins Bloomberg School of Public Health. The study, published this week in the International Journal of Men’s Health, looks at the direct and indirect costs associated with health inequalities and projects the potential cost savings of eliminating these disparities for minority men in the U.S.
“Health disparities have a devastating impact on individuals and families, and they also affect society as a whole,” said Roland J. Thorpe, Jr., PhD, lead author of the study and Assistant Professor at the Johns Hopkins Bloomberg School of Public Health and Director of the Program for Research on Men’s Health in the Johns Hopkins Center for Health Disparities Solutions. “Quantifying the economic impact of health inequalities among men highlights how enormous a societal problem this is.”
Researchers used data from the Agency for Health Care Research and Quality’s 2006-2009 Medical Expenditure Panel Survey (MEPS) to determine the prevalence of a variety of health statuses and conditions (for example, fair/poor health, obesity, diabetes, heart disease) among each racial/ethnic group (African American, Asian, Hispanic and white). This information was incorporated in statistical models to estimate the total direct medical costs and the proportion of costs incurred due to health disparities for each group. The direct medical expenditures for African-American men over the four-year period totaled $447.6 billion; and 5.4 percent, or $24.2 billion, were excess costs attributed to health disparities. There were no excess direct costs due to health disparities for the other racial/ethnic groups over the four year period.
The indirect costs of lower worker productivity due to illness and premature death were calculated using data from MEPS and the CDC’s National Vital Statistics System. Over the four-year period, these factors cost the economy a total of $436.3 billion—lower worker productivity due to illness contributed $28 billion in excess costs, and premature death contributed $408.3 billion. Of the total indirect costs, African-American men accounted for $317.6 billion, or 72 percent; indirect costs totaled $115 billion for Hispanic men and $3.6 billion for Asian men.
“These stark findings underscore the fact that we can’t afford to overlook men’s health disparities that exist in this country,” added Thorpe. “The cost to society—both moral and economic—is staggering.”
Related articles

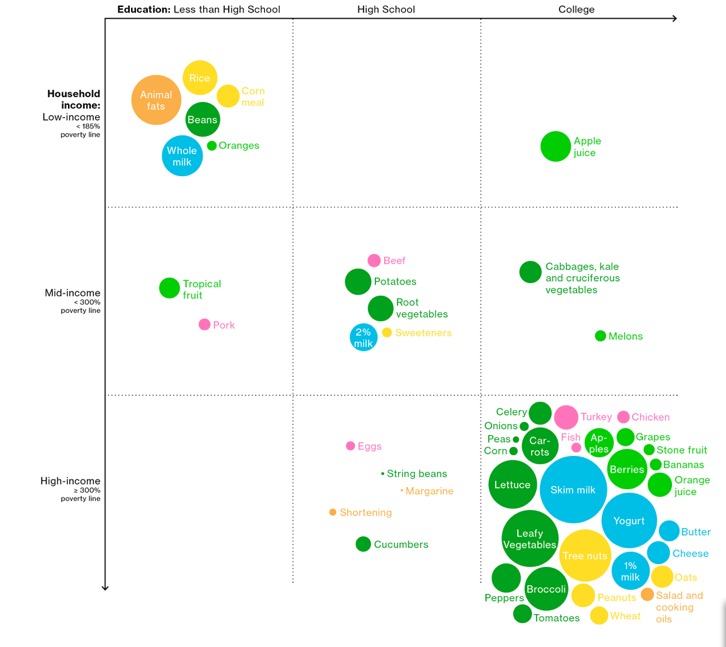
[Repost] You Are What You Eat, and You Eat What You Earn
From the November 2013 Bloomberg article
There are plenty of reasons why Americans eat the foods they do, but two of the most important factors in determining diets are income levels and education.
An analysis of data from the U.S. Department of Agriculture reinforces the notion that high earners with college degrees are more likely than other Americans to eat a healthy diet. In the opposite corner, lower-income Americans without high school degrees are more likely to drink whole milk and eat beans cooked with animal fats. Still, it’s hard to explain the divide between orange juice (high-income college grads), apple juice (low-income college grads), and whole oranges (low-income, less than a high school diploma).

[Reblog] Social inequality: A blind spot for health reporters
Joe Rojas-Burke is AHCJ’s core topic leader on the social determinants of health. To help journalists broaden the frame of health coverage to include factors such as education, income, neighborhood and social network, Rojas-Burke will hunt for resources, highlight excellent work and moderate discussions with journalists and experts. Send questions or suggestions to joe@healthjournalism.org or tweet to @rojasburke.
Dozens of news stories over the past year have reported on the disturbing data showing that Americans are dying younger than people in other wealthy countries and falling behind in many other measures of population health.
But much of the reporting I’ve seen shies away from covering a crucial part of the story: How social inequality may be the most important reason why the health status of Americans is failing to keep up with progress elsewhere.
Being born into poverty, growing up with curtailed opportunities for education and employment, living in a disadvantaged neighborhood – these social determinants of health are like the cards you’re dealt in a game of poker. It’s hard to win if the deck is stacked against you.
Researchers in sociology and public health have developed a fair amount of evidence that social status (typically measured by income or education) may be the most significant shaper of health, disability and lifespan at the population level. In the picture that is emerging, social status acts through a complicated chain of cause-and-effect. Education equips people with knowledge and skills to adopt healthy behaviors. It improves the chances of securing a job with healthy working conditions, higher wages, and being able to afford housing in a neighborhood secure from violence and pollution. The job security and higher income that tend to come with more education provide a buffer from chronic stress – a corrosive force that undermines health among lesser educated, lower income people. Research consistently shows that more education gives people a greater sense of personal control. Positive beliefs about personal control have a profound impact on how people approach life, make decisions about risky behavior, and cope with illness.
Since 1980, virtually all gains in life expectancy in the U.S. have occurred among highly educated groups. In a revealing analysis published in 2008, researchers looked at long-term changes in infant mortality and adult deaths before age 65 and found a widening gap between haves and have-nots over the past 30 years. If all people in the U.S. population experienced the same health gains as the most advantaged, they found that 14 percent of the premature deaths among whites and 30 percent of premature deaths among people of color would have been prevented.
But news outlets seem almost afraid to dig into questions about social inequality. Take, for example, CNN’s coverage of the Institute Of Medicine’s “Shorter Lives, Poorer Health” report in January. The IOM experts examined many measures in which the United States is lagging behind gains in other nations: infant mortality, disabilities, homicides, teen pregnancy, drug-related deaths, obesity, prevalence of AIDS, and life expectancy.
When the CNN coverage got around to explaining likely causes, it tossed out a range of possibilities, most of them blaming individual behavior. Compared with other wealthy nations we eat too much, spend more time driving than walking, fail to use seat belts, abuse more drugs, and use guns to shoot each other more. In the middle of this laundry list, the CNN report makes a glancing reference to the social determinants of health: “Americans benefit much less from social programs that could negate the effects of poverty.”
In July, a headline-garnering paper in the Journal of the American Medical Association explained how the U.S. lapsed from 20th to 27th among wealthy nations in terms of life expectancy at birth, and from 18th to 27th in terms of premature deaths.
…
Related articles
- Social Determinants of Health (ajpmonline.wordpress.com)
- Social Determinants of Health: Us and Them (ajpmonline.wordpress.com)
- [News article] Britain’s poor ‘will die before they retire’ if pension reforms aren’t matched by health improvements (jflahiff.wordpress.com)
- The poor die young – in Leeds as in the rest of the UK. The injustice of the Coalition’s pension proposals. (leedsnwclp.wordpress.com)
- World Health Organisation: unemployed youth in Britain are a public health time bomb (telegraph.co.uk)
- New Evidence on Social Isolation and Mortality (inequalitiesblog.wordpress.com)
- Britain told social inequality has created ‘public health timebomb’ (theguardian.com)
- Collapsing civilization: Britain told social inequality has created ‘public health timebomb’ (sott.net)
- Three Theories of Health and the Mortality Shift (healthandeverythingblog.wordpress.com)
[News article] Britain’s poor ‘will die before they retire’ if pension reforms aren’t matched by health improvements
From the 6 December 2013 article at The Independent
Thousands of Britain’s poorest people “will be dead before they can retire” if sweeping pension reforms are not matched by urgent action on health inequalities between rich and poor, experts have said.
Plans to raise the basic state pension age to 70 for people currently in their twenties were laid out in the George Osborne’s Autumn Statement this week. But with male life expectancy at birth as low as 66 in some of the most deprived parts of the country, public health experts have warned that a “one size fits all” pension age risks condemning many to a life without retirement.
Average UK life expectancy at birth was 78.2 in 2010. Nationally, the figure is increasing, but huge variations exist and progress has been slower in deprived communities where poverty leads to poor diets, smoking rates are higher and alcohol abuse more common.
In Glasgow City, where male life expectancy at birth is 71.6, boys born in 2010 are expected to die on average 13.5 years earlier than those born in the London borough Kensington and Chelsea, where life expectancy is 85.1. Girls in born in the London borough in 2010 can expect 12 more years of life than those in Glasgow. Even these figures veil vast inequalities that exist within regions, with life expectancies as low as 66 years in some of Glasgow’s most deprived areas.
Martin McKee, professor of European Public Health at the London School of Hygiene and Tropical Medicine, and fellow of the Faculty of Public Health, said that if the Government wanted to raise the pension age, they must first tackle health inequalities.
“George Osborne is thinking about the average life expectancy. The average life expectancy is fairly meaningless if you’re living in a former coal mining village in Nottinghamshire or in inner-city Glasgow,” he toldThe Independent. “There are many parts of the country where people have nowhere near the average life expectancy and, crucially, nowhere near the average healthy life expectancy. It’s not just the fact people will be dead before they reach pensionable age, it’s that they will be unfit to work.”
David Walsh, a public health expert at the Glasgow Population Health Centre said that a single pension age across all areas of the country was “at the very least problematic”.
…
Related articles
- Britain’s Poor Will Die Before They Retire (sorendreier.com)
- Britain’s poor ‘will die before they retire’ if pension reforms aren’t matched by health improvements (engineeringevil.com)
- Living Longer…and Longer…. (worthwhile.typepad.com)
- Work until you’re 70: Chancellor George Osborne accused of ‘living in fantasy land’ over Autumn Statement pension reforms (independent.co.uk)
- Ever receding retirement? (centrallobby.politicshome.com)
- State pension: age-old problems | Editorial (theguardian.com)
[News Report] Cuts to Local Health Departments Hurt Communities
From the 14 November 2013 Science Daily Report
Local health departments (LHDs) can play pivotal roles in U.S. communities by helping to link people with medical services and assuring access to care when it is otherwise unavailable. However, a new study in the American Journal of Preventive Medicine finds that many LHDs aren’t able to meet these goals, which could spell trouble for the uninsured and underinsured.
“Our report shows that in 2010, about 28 percent of LHDs had not conducted any of the three targeted activities in our study,” which looked at how LHDs assessed gaps in care, increased access to health services and used strategies to meet the health needs of the underserved, said lead author Huabin Luo, Ph.D, former research fellow with the Centers for Disease Control and Prevention and assistant professor in the department of public health at the Brody School of Medicine at East Carolina University.
http://www.sciencedirect.com/science/article/pii/S074937971300487X
In recent years, deep funding cuts have impacted local health departments. For example, between 2008 and 2009 alone, over 23,000 LHD jobs were eliminated. This combined with an increase in demand for health care services can mean an increase in health disparities for those who rely on community health care.
The study found that LHDs with larger budgets in bigger population centers were more likely to provide access to health services compared to smaller LHDs with fewer financial resources, where they may be needed more.
…
Hanen noted that as health insurance coverage becomes more widespread, LHDs will continue to identify and link people without health insurance to programs that provide health care services. “It cannot be overstated enough that poor housing, education, low income, unemployment and lack of transportation in a neighborhood are all interconnected and are all factors that determine health.”

Related articles
- Cuts to Local Health Departments Hurt Communities (publichealthwatch.wordpress.com)
- Health cuts hurt inspections, but flu programs OK (news-journalonline.com)
- Health department warns of scam targeting restaurants (wkyt.com)
- Erie County Council discusses merging health, human services departments (goerie.com)
[JAMA Perspective] Dead Man Walking
Whether one is for or against all or parts of Obamacare, surely, we as a country can do better in providing needed health care to the poor, especially the poorest of the poor.
Excerpts from the November 2013 JAMA article by Michael Stillman, M.D., and Monalisa Tailor, M.D.
…For many of our patients, poverty alone limits access to care. We recently saw a man with AIDS and a full-body rash who couldn’t afford bus fare to a dermatology appointment. We sometimes pay for our patients’ medications because they are unable to cover even a $4 copayment. But a fair number of our patients — the medical “have-nots” — are denied basic services simply because they lack insurance, and our country’s response to this problem has, at times, seemed toothless.
In our clinic, uninsured patients frequently find necessary care unobtainable. An obese 60-year-old woman with symptoms and signs of congestive heart failure was recently evaluated in the clinic. She couldn’t afford the echocardiogram and evaluation for ischemic heart disease that most internists would have ordered, so furosemide treatment was initiated and adjusted to relieve her symptoms. This past spring, our colleagues saw a woman with a newly discovered lung nodule that was highly suspicious for cancer. She was referred to a thoracic surgeon, but he insisted that she first have a PET scan — a test for which she couldn’t possibly pay.
However unconscionable we may find the story of Mr. Davis, a U.S. citizen who will die because he was uninsured, the literature suggests that it’s a common tale. A 2009 study revealed a direct correlation between lack of insurance and increased mortality and suggested that nearly 45,000 American adults die each year because they have no medical coverage.1 And although we can’t confidently argue that Mr. Davis would have survived had he been insured, research suggests that possibility; formerly uninsured adults given access to Oregon Medicaid were more likely than those who remained uninsured to have a usual place of care and a personal physician, to attend outpatient medical visits, and to receive recommended preventive care.2 Had Mr. Davis been insured, he might well have been offered timely and appropriate screening for colorectal cancer, and his abdominal pain and obstipation would surely have been urgently evaluated.
…
Related articles
- With no insurance, he used enemas to treat colon cancer. Now he’s going to die. (americablog.com)
- Healthcare Costs Driven By High Device, Drug Prices: Researchers (huffingtonpost.com)
Public Health Policies, Practices May Negatively Affect Marginalized Populations
From the 31 October 2013 Science Daily article
Despite the best intentions of those working in public health, some policies and practices inadvertently further disadvantage marginalized populations, according to a commentary by a researcher at St. Michael’s Hospital
Dr. Diego S. Silva, a scientist in the hospital’s Centre for Research on Inner City Health, said there’s an emphasis toward social justice in public health, particularly when it comes to people who are marginalized, disadvantaged or vulnerable.
“For example, despite evidence suggesting that people who are homeless are at greater risk of being infected with influenza and suffer greater morbidity than the general population, many pandemic influenza plans provide impracticable advice or otherwise fail to address their specific needs,” said Dr. Silva.
The commentary appears online today in the Canadian Journal of Public Health.
New Report: Call for President Obama Urged to ‘Remove Public Veil of Ignorance’ Around State of US Health

View larger map at http://gamapserver.who.int/mapLibrary/Files/Maps/PerCapitaUSD_2011.png
From the 29 August 2013 Science Daily article
In a call to action on the sorry comparative state of U.S. health, researchers at Columbia University’s Mailman School of Public Health are urging President Obama to “remove the public veil of ignorance” and confront a pressing question: Why is America at the bottom? The report, published in the journal Science, appeals to the President to mobilize government to create a National Commission on the Health of Americans. The researchers underscore the importance of this effort in order for the country to begin reversing the decline in the comparative status of U.S. health, which has been four decades in the making.
This is not a challenge that can be left to private groups, no matter how well meaning. Drs. Ronald Bayer and Amy Fairchild, both Professors of Sociomedical Sciences, argue, “The health status of Americans is a social problem that demands social solutions.” More is at stake than the U.S. healthcare system, which fails to provide needed care to millions of Americans. “There is a need for bold public policies that move beyond individual behavior to address the fundamental causes of disease,” Bayer and Fairchild conclude.
A January 2013 report by the U.S. National Research Council (NRC) and Institute of Medicine (IOM) ranks the United States last among peer nations in health status and compares it unfavorably to 17 peer countries at almost every stage of the life course. The report, titled “U.S. Health in International Perspective: Shorter Lives, Poorer Health,” emphasizes that socioeconomic causes are the drivers of these outcomes and details the categories in which the U.S. has the worst or next-to-worst results:
- The U.S. has higher rates of adverse birth outcomes, heart disease, injuries from motor vehicle accidents and violence, sexually acquired diseases, and chronic lung disease.
- Americans lose more years of life to alcohol and other drugs.
- The U.S. has the highest rate of infant mortality among high-income countries.
- The U.S. has the second highest incidence of AIDS and ischemic heart disease,
- For decades, the U.S. has experienced the highest rates of obesity in children and adults as well as diabetes from age 20 and up.
Related articles
[Reblog] Futuristic Private Patient Rooms and Low-Tech Health Innovation: The Battle
Futuristic Private Patient Rooms and Low-Tech Health Innovation: The Battle.
Whenever I give an interview about the future of medicine and current global trends, the question whether wealthier people would have even better care always comes up. Obviously, this is a crucial issue. But I take it to a next level. In the future, not just richer people will get better care but will also have a chance to become superhuman by implanting and using expensive medical innovations from augmented reality-based contact lenses to artificial organs.
Although, there will always be a battle between the major motivation behind creating better experience for the rich (money) and the motivation behind designing innovations for underdeveloped areas (providing better care).
It might not be the best comparison, but take a look at the Patient Room 2020 design (photo below) and a non-profit model for fostering low-tech health innovation. The room looks great and is certainly comfortable but it lacks of real innovation.
Regarding fostering low-tech innovation, there is an amazing initiative in Seattle.
Anurag Mairal, director of technology solutions at PATH Health Technologies, says that it’s time to start looking at low-cost innovations in healthcare differently. What should the road map be for an innovation? Should the product debut in a developing country first and then, evolve for the developed market or vice versa?
Examples include river blindness tests, mobile-phone milk pasteurization (picture below) and female condoms.
We should find a balance between high-class and low-tech innovations in order to provide better care either for developed or underdeveloped areas.
Related article
- How to Foster Low-Tech Health Innovation (The Atlantic)
George W. Bush’s angioplasty: Did he receive the best care? (With Lively Discussion on Pros/Cons of Medical Screening)

Polygon Medical Animation – Angioplasty Procedure (Photo credit: Polygon Medical Animation)
From the 19 August 2013 Kevin MD article by ALBERT FUCHS, MD
…..
The press coverage of Bush’s angioplasty had frequent questions about the necessity of the angioplasty and the cost of such a procedure. That is precisely not the point, and gives the public the incorrect idea that angioplasties are expensive and beneficial luxuries. BMWs, after all, are unnecessary and expensive, but very nice. And if a VIP gets something unnecessary and expensive, shouldn’t I want one too? The point of the evidence about angioplasties is that in most patients they have no benefit. Focusing on “necessity” misses that point.
It is entirely possible that Bush’s care was flawless. One possibility was that his stress test was extremely abnormal. Such very abnormal tests were excluded from the COURAGE trial, and we have no definitive evidence whether medications or stenting is best in those cases.
The important thing for the public to understand is that VIPs sometimes get terrible care. I’ve personally seen that myself. Physicians often over-test and over-treat celebrities, wrongly thinking that this will protect them from blame for any adverse outcome later. It’s much easier to tell a prominent patient that we will fix your problem with a high-tech and very expensive solution, rather than taking the time to educate the patient that we should start a few very old and very inexpensive medicines which have been proven to save lives. Paradoxically, we’re frequently much more comfortable doing the right thing for patients who will not draw public attention.
……
The comments section was very interesting and lively.
Pap testing was one topic. An excerpt
For those women interested, in my opinion, the best screening program in the world for cervical cancer is the new Dutch program. They’ll scrap their 7 pap test program, 5 yearly from 30 to 60, and offer instead 5 hrHPV primary tests at ages 30,35,40,50 and 60 and ONLY the roughly 5% of women who are HPV+ and at risk will be offered a 5 yearly pap test. (until they clear the virus) This will save more lives and take most women out of pap testing and harms way. (damage to the cervix can mean miscarriages, premature babies, c-sections etc.)
Those HPV- and no longer sexually active or confidently monogamous might choose to stop all further testing. Dutch women are already using a HPV self-test option/device, the Delphi Screener. (also, available in Singapore and elsewhere)
I’ve also, declined breast screening even though that cancer is far more common. Weighing up the risks and actual benefits, it doesn’t get over the line for me. (The Nordic Cochrane Institute brochure on breast screening and Professor Michael Baum’s informative articles and lecture helped me make an informed decision to decline testing)Speaking generally:
We need to stop telling women what to do and start respecting informed consent. Give women real information on risk and ACTUAL benefit, respect them as competent adults/individuals and offer evidence-based testing that focuses on what’s best for them AND, leave the final decision to women, to accept or decline screening as they see fit.
Related Resources (just a few from many!)
- Cochrane Reviews (require subscription, available at many academic/health science libraries…however free summaries are here)
systematic reviews of primary research in human health care and health policy, and are internationally recognised as the highest standard in evidence-based health care. They investigate the effects of interventions for prevention, treatment and rehabilitation. They also assess the accuracy of a diagnostic test for a given condition in a specific patient group and setting. They are published online in The Cochrane Library.
Example of a free summary
Screening for breast cancer with mammography (2013) –[scroll down for link to abstract]
- AHRQ-Patient Involvement
- Evaluating Health Information (with links)
- Research papers summarized for us all (links to resources)
- Evidence based practice (LibGuide with links to tutorials, databases, web resources and more)
- Crunching Numbers: What Cancer Screening Statistics Really Tell Us (National Cancer Institute)
- AHRQ-For Professionals-Prevention and Chronic Care
- Evidence Based Decision Making
- US Preventive Services Task Force
- What Not to Do in Primary Care: Overuse of Preventive Services (
 Microsoft PowerPoint version – 1.12 MB )
Microsoft PowerPoint version – 1.12 MB )
Michael LeFevre, University of Missouri-Columbia
- What Not to Do in Primary Care: Overuse of Preventive Services (
- US Preventive Services Task Force
- Evidence Based Decision Making
Related articles
- UDoTest, HPV Virus Home Screening Kit, Launches In South Africa; Doctor Says It’s ‘More Effective Than A Pap Smear’ (medicaldaily.com)
- Many Docs Don’t Follow HPV/Pap Test Guidelines (nlm.nih.gov)
- Women may not need pap smears every two years according to University of NSW research (abc.net.au)
- Outdated practice of annual cervical-cancer screenings may cause more harm than good (eurekalert.org)
- Why Some Parents Are Refusing HPV Vaccine For Their Children (shotofprevention.com)
- On Self-Advocacy and Paying It Forward (draemadden.wordpress.com)
[Reblog]The rich really are different: Their bodies contain unique chemical pollutants

Disparity of rich and poor in Rio de Janeiro (Photo credit: Wikipedia)
From the 5 August 2013 article at Quartz by Christopher Mims
“Tell me what kinds of toxins are in your body, and I’ll tell you how much you’re worth,” could be the new motto of doctors everywhere. In a finding that surprised even the researchers conducting the study, it turns out that both rich and poor Americans are walking toxic waste dumps for chemicals like mercury, arsenic, lead, cadmium and bisphenol A, which could be a cause of infertility. And while a buildup of environmental toxins in the body afflicts rich and poor alike, the type of toxin varies by wealth.
America’s rich are harboring chemicals associated with what are normally considered healthy lifestyles
People who can afford sushi and other sources of aquatic lean protein appear to be paying the price with a buildup of heavy metals in their bodies, found Jessica Tyrrell and colleagues from the University of Exeter. Using data from the US National Health and Nutrition Examination Survey, Tyrrell et al. found that compared to poorer people, the rich had higher levels of mercury, arsenic, caesium and thallium, all of which tend to accumulate in fish and shellfish.
The rich also had higher levels of benzophenone-3, aka oxybenzone, the active ingredient in most sunscreens, which is under investigation by the EU and, argue some experts, may actually encourage skin cancer.
America’s poor have toxins associated with exposure to plastics and cigarette smoke
Higher rates of cigarette smoking among those of lower means seem to be associated with higher levels of lead and cadmium. Poor people in America also had higher levels of Bisphenol-A, a substance used to line cans and other food containers, and which is banned in the EU, Malaysia, South Africa, China and, in the US, in baby bottles.
Previous research has established that rich Americans are more likely to eat their fruits and vegetables and less likely to eat “energy-dense” fast food and snacks, but this work establishes that in some ways, in moving up the economic ladder Americans are simply trading one set of environmental toxins for another.
Related articles
- The rich really are different: Their bodies contain unique chemical pollutants (pitrejeanclaude.wordpress.com)
- The rich really are different: Their bodies contain unique chemical pollutants (rahconteur.wordpress.com)
- You Are Your Net Worth: How Toxins Found in the Rich and Poor Differ (theatlanticwire.com)
- Chemicals in Our Bodies Can Predict How Rich or Poor We Are (motherboard.vice.com)
- Rich people’s bodies are polluted with different, more expensive toxins (grist.org)
- Blood Samples can Tell If You Are Rich or Poor: Study (natureworldnews.com)
- Chemical Build-Up in the Body Affecting People from All Income Groups (medindia.net)
- Study: Money Doesn’t Protect People From Toxicants, Just Changes Them (webpronews.com)
- How the chemicals in your blood can betray your wealth (talesfromthelou.wordpress.com)
Life Expectancy Shortest In Southern ‘Poverty Belt’ (INFOGRAPHIC)
From the 19 July post at HuffPost
Living in a high-poverty area often means a lifetime of struggle with underperforming public schools, limited job opportunities, higher crime rates, and poor nutrition, health care and housing — all of which can add up to a shorter, sicker retirement.
Americans who live in the South can expect to live fewer healthy years past 65 than those who live in other parts of the country, according to a new report from the CDC. Health disparities among seniors in their final years align closely with profound geographical differences in poverty. The region where more than 30 percent of people live in high-poverty areas — dubbed the “poverty belt” by The Atlantic’s Richard Florida, falls right over the states with the lowest healthy life expectancies. As inequality in the U.S. climbs steadily, this public health crisis may only expand.
From the US Centers for Disease Control and Prevention site

Related articles
- This Infographic Proves That Republican Policies Kill People (IMAGE) (addictinginfo.org)
- CDC: Retirement Shorter, Sicker In Southern States (atlanta.cbslocal.com)
- Golden years shorter, sicker in Southern states (kfwbam.com)
- South lags in state-by-state study of life expectancy for seniors (cbsnews.com)
- Healthy Life Expectancies at Age 65 Highest in Hawaii, Lowest in Mississippi (cdc.gov)
- Mind The Gap: Mapping Life Expectancy By Subway Stop (fastcoexist.com)
- Life Expectancy Gap Between Black And White Populations Affected By Heart Disease And Homicide (hngn.com)
HIGHLIGHTED STORIES:Los Angeles ‘Health Atlas’ Show Alarming Disparities Between Neighborhoods
“More than 100 health indicators — such as obesity, coronary disease and asthma — were studied within neighborhoods across Los Angeles and compiled into a health atlas, which includes a series of 115 maps. Results show that while economic disparities do affect health, so does land use. The atlas was released by former Mayor Antonio Villaraigosa on his last day in office.
“Too often a person’s neighborhood determines their health destiny,” Villaraigosa said. The goal of compiling the atlas, he noted, was to ensure that city officials would consider how future development impacts neighborhoods where bike lanes, walking paths and parks could be integrated with new housing developments and transportation hubs.”
 In addition to socioeconomic disparities, the proximity of parks, walking paths and bike lanes affects the health of residents of Los Angeles. This correlation was discovered when 100 health indicators (including obesity, coronary heart disease, and asthma) were studied in neighborhoods across Los Angeles and compiled into a “health atlas.” Former mayor Antonio Villaraigosa is passing this information to the new mayor, Eric Garcetti, in the hopes that city departments will consider the importance of reducing environmental disparities in future development.
In addition to socioeconomic disparities, the proximity of parks, walking paths and bike lanes affects the health of residents of Los Angeles. This correlation was discovered when 100 health indicators (including obesity, coronary heart disease, and asthma) were studied in neighborhoods across Los Angeles and compiled into a “health atlas.” Former mayor Antonio Villaraigosa is passing this information to the new mayor, Eric Garcetti, in the hopes that city departments will consider the importance of reducing environmental disparities in future development.
Read More at: http://www.huffingtonpost.com/2013/07/08/los-angeles-health-atlas_n_3557778.html
The U.S. Health Disadvantage – Part 2: Possible Causes and Solutions
by Kirsten Hartil
“Everyone has the right to a standard of living adequate for the health and well-being of himself and his family, including food, clothing, housing and medical care.”
At least according to Article 25 of The United Nations Universal Declaration of Human Rights, so why does the United States, one of the wealthiest countries in the world, have some of the poorest health outcomes compared to other high income countries?
My previous blog, adapted from the Institute of Medicine (IOM) report U.S. Health in International Perspective: Shorter Lives, Poorer Health, described how the U.S. compares in causes of mortality and years of life lost with other high income and OECD countries. Here, as outlined in the report, I explore some of the social determinants of health that may explain this. Social determinants of health, as opposed to biological determinants (biology and genetics), describe the…
View original post 1,307 more words
Pre-Teen Health Disparities
Logo of the United States National Library of Medicine. (Photo credit: Wikipedia)
From the (NLM) Director’s comments page
Greetings from the National Library of Medicine and MedlinePlus.gov
Regards to all our listeners!
I’m Rob Logan, Ph.D. senior staff National Library of Medicine for Donald Lindberg, M.D, the Director of the U.S. National Library of Medicine.
Here is what’s new this week in MedlinePlus.
Harmful health behaviors and experiences are significantly more likely among African-Americans and Hispanic-Americans than white fifth-graders, suggests a pioneering health disparities study recently published in The New England Journal of Medicine.
In a study of 5,119 randomly selected public school fifth-graders (and their parents) in three U.S. cities, 20 percent of African-American fifth-graders witnessed a threat or injury with a gun compared to 11 percent of Latinos and five percent of white youngsters.
Several of the study’s 16 measures consistently suggest unhealthy experiences were more likely to occur among African-American and Hispanic American fifth-graders while therapeutic actions were more likely to happen to white peers.
For example, while white fifth-graders exercised vigorously an average of four and a half days per week, Latino youngsters exercised about 3.77 days and African-American fifth-graders vigorously exercised about three and a half days each week. All the above differences are statistically significant.
The authors assessed other unhealthy experiences including victimization by peers and unhealthy behaviors such as alcohol use. The authors evaluated other therapeutic behaviors including bike-helmet use…

Continue reading the transcript here
OR
Listen to the message here –>podcast100812.mp3
Related articles
- New Study Shows School has Large Role in Kids’ Health Disparities (cityconnectsblog.wordpress.com)
Analysis Of Interventions In 5 Diseases Offers Guidelines To Help Close The Gap
Racial/Ethnic Disparities in Self-Rated Health Status among Adults with and Without Disabilities — United States, 2004–2006. MMWR 2008:57(39);1069-1073.

From the 19th July 2012 article at Medical News Today
Major disparities exist along racial and ethnic lines in the United States for various medical conditions, but guidance is scarce about how to reduce these gaps. Now, a new “roadmap” has been unveiled to give organizations expert guidance on how to improve health equity in their own patient populations.
Finding Answers, a national program based at the University of Chicago and funded by the Robert Wood Johnson Foundation, seeks evidence-based solutions to reduce racial and ethnic health disparities. Its new roadmap, outlined as part of a symposium of six papers published in the Journal of General Internal Medicine (JGIM), builds upon seven years of administering grants, reviewing literature, and providing technical assistance to reduce health disparities.
The roadmap’s architects hope it can provide direction on creating effective and sustainable interventions as the health disparities field shifts from measuring the problem to taking action. ..
…The paper highlights the initial need for recognizing disparities and commitment to their reduction, and suggests that programs to reduce disparities should be integrated into broader quality improvement efforts at clinics, hospitals and other health systems.
“In the past, people did disparities work or quality work, but the two wouldn’t touch one another,” Chin said. “We’re merging the quality improvement field and the disparities field.”
The roadmap also contains advice on designing interventions to address disparities, drawing upon systemic reviews of disparities research in various diseases. Five such reviews – on HIV,colorectal cancer, cervical cancer, prostate cancer and asthma – accompany the roadmap article in the JGIM symposium.
Researchers identified characteristics of successful interventions across the five new articles and previously published reviews of cardiovascular disease, diabetes, depression and breast cancer. Effective projects were found to utilize team approaches to care, patient navigation, cultural tailoring, collaboration with non-health care partners such as families or community members, and interactive skill-based training.
The reviews also identified potential targets for reducing health disparities that have yet to be examined..
..While offering general guidelines for best practices, the authors point out that the specifics of any organization’s effort to reduce disparities must be custom-fit to the patient population and community. …
References for this article
The paper, “A Roadmap and Best Practices for Organizations to Reduce Racial and Ethnic Disparities in Health Care,” was published on July 13 by the Journal of General Internal Medicine. Five systematic reviews of disparities interventions in HIV, colorectal cancer, cervical cancer, prostate cancer and asthma accompany the main article. The articles are open access, and can be read here:http://www.springerlink.com/content/0884-8734/27/8/
The publications were funded by Finding Answers: Disparities Research for Change, a Robert Wood Johnson Foundation program, with direction and technical assistance from the University of Chicago. More information about Finding Answers and the Roadmap to Reduce Disparities can be found athttp://www.solvingdisparities.org.
University of Chicago Medical Center
Related articles
- New roadmap suggests proven routes to ending health disparities (eurekalert.org)
- New roadmap suggests proven routes to ending health disparities (medicalxpress.com)
- Researchers highlight the impact of slavery on health and disease (blogs.nature.com)
- Racism’s Hidden Toll (innerstandingisness.wordpress.com)
- Health Disparities and Student Learning: Taking Action for Wellness (healthyschoolscampaign.typepad.com)
- Better-Educated Blacks, Lower Odds of Hypertension (nlm.nih.gov)
- Reducing Geriatric Deaths From Chronic Illnesses With The Help Of A Nursing Program (medicalnewstoday.com)
- Health Disparities and Student Learning: Taking Action for Wellness (innerstandingisness.wordpress.com)
- ECRI Institute Identifies 1,000 Interventions for AHRQ Healthcare Horizon Scanning System (sacbee.com)
- An Opportunity for Small Communities to Solve Big Health Problems (thefergusongroup.typepad.com)
- “Telemedicine Critical for Latino Health” The National Latino Alliance on Health Information Technology Advisor Dr. Elena Rios (listahit.wordpress.com)
Migrant Health Clinics Caught In Crossfire Of Immigration Debate

THE CHILDREN OF MIGRANT WORKERS PLAY MARBLES WHILE THEIR PARENTS WORK IN FIELDS – NARA – 543855 (Photo credit: Wikipedia)
From a 6 June 2012 article at Kaiser Health
..clinics [which are] part of a 50-year-old federally funded program to treat migrant and seasonal farmworkers, have become the latest flash points in the national immigration debate. Health center officials across the country describe how local, state and national law enforcement authorities have staked out migrant clinics, detained staff members transporting patients to medical appointments and set up roadblocks near their facilities and health fairs as part of immigration crackdowns…
…
“We are looking at a growing climate of fear where folks really think long and hard about accessing basic services,” says Milton Butterworth, who oversees outreach migrant health services for Blue Ridge Community Health Services in Hendersonville, N.C.
Even many legal workers do not seek care at the health centers because they are fearful of exposing family members who are not legal residents, says Tara Plese, a spokeswoman for the Arizona Association of Community Health Centers. “There is a big fear factor and it’s a big concern from a public health perspective.”
Those concerns include making sure farmworkers’ children are vaccinated, stopping the spread of infectious diseases like AIDS and treating those with chronic problems such as diabetes, officials say. Many farmworkers avoid seeking care except in emergencies.
Federal Aid Opposed
Supporters of the nation’s 156 migrant clinics, which are typically part of community health centers, say caring for all farmworkers helps protect them as well as the public — and is a humane way to treat three million people toiling at the heart of the nation’s food supply. About half of those are illegal immigrants, according to the latest federal survey of agricultural workers conducted in 2009.
“Migrant health centers continue to help ensure the safety of the nation’s food supply by keeping those who harvest it healthy,” …
Related articles
- Fear keeps migrant workers from getting health care (usatoday.com)
- Alessandro Penso, Migrant Workers (mastersofphotography.wordpress.com)
Social Factors May Affect Lifespan More Than Race, Location
A group of socioeconomic factors such as education, income and work are better indicators of your chances of living to age 70 than race or geography, a new study shows.
The findings challenge the long-held belief that race or the region of the country where you reside are the best markers of how long you may live, according to researchers from Stanford University School of Medicine in Stanford, Calif.
Previous research has found large differences in life expectancy in various regions of the United States. For example, people tend to die younger in large urban areas and in the South. A study published last year found that men in five counties in Mississippi lived an average of 66.5 years, several years less than the national average of 75.4 years for men.
Racial disparities also are a well-established factor in life expectancy. For example, a recent study found that white men live an average of about seven years longer than black men, and white women live about five years longer than black women, according to a Stanford University news release.
In the new study, the researchers examined data on the probability of survival to age 70 for people in counties across the United States. The data was initially categorized according to sex and race, but the researchers then considered how other factors affect life expectancy.
The analysis showed that when factors related to local social conditions — such as education, income, and job and marital status — are included, health differences based on race and region virtually disappear….
Related articles
How Smartphones Could Impact Public Health
 (Chart via Pew.)Smartphone owners now outnumber regular cell phone owners for the first time, according to a new study.
(Chart via Pew.)Smartphone owners now outnumber regular cell phone owners for the first time, according to a new study.
From the March 3, 2012 article in the Boston Globe
…
This smartphone proliferation has tremendous potential from a public health perspective. When Ispoke with Frank Moss at Bluefin Labs for the story, he described a day when doctors would simultaneously prescribe medicine with an app to help patients better monitor their care (you can read more of Moss’s ideas about mobile health in his New York Times op-ed). When you consider that smartphone penetration is already higher in African American and Latino communities (49 percent in each group vs. a national average of 46 percent) and that these two groups are historically disadvantaged when it comes to accessing health care (just browse the February headline roundup from the Kaiser Family Foundation for examples of these disparities), it would be revolutionary to begin targeting health care apps and devices to these populations.
When we consider looking that the gadgets being pushed into the marketplace to help us monitor our health (many of which I tried while reporting the story) we forget that they’re all targeting ”fairly affluent people,” says Jane Sarasohn-Kahn, a health economist who often blogs about public health at Health Populi. “When we look at the burden of chronic disease, it’s the African Americans and Latinos, the poor and less-educated, and very old or very young that don’t have access to healthy food or safe places. These populations have spent as much money on their mobile phones [as the rest of the country], but the platform technology hasn’t penetrated into poor urban areas.”
Sarasohn-Kahn hopes that Medicaid will start developing applications to target these populations, and points to the recent move by a former CDC scientist to develop an asthma inhaler outfitted with GPS and Wifi enabled sensors. When distributed in urban populations, the inhalers allow the doctors to better track their patients, and allow epidemiologists to learn more about the health of these groups. Right now, the smartphones are spreading at a rapid clip through the country. We just need to be smart enough to know how to help them nudge us all toward better health….
Study takes aim at education-based death rate disparities
From the 15 December 2011 news release via Eureka alerts
WASHINGTON, DC — A study in the December issue of the American Sociological Review has brought new understanding as to why death rates for less educated middle aged adults are much higher than for their more educated peers despite increased awareness and treatments aimed at reducing health disparities.
[Full text of the article The Enduring Association between Education and Mortality: The Role of Widening and Narrowing Disparities is free at http://asr.sagepub.com/content/76/6/913.full.pdf+html
Click here for the accompanying 7 minute interview podcast. The author talks about the findings in his work, implications, and touches on the processes of doing the research and writing the paper. The author comes across as knowledgeable, reflective, willing to learn from others, grateful for financial support, and driven to share his knowledge for the benefit of all]
For decades, data has shown that middle aged adults with low education levels—that is high school or less—are twice as likely to die as those with higher education levels. Professor Richard Miech, of the Department of Health and Behavioral Sciences at the University of Colorado Denver’s College of Liberal Arts and Sciences, and his colleagues wanted to better understand why this persists. They found that as new causes of death emerge, people with lower education levels are slower to respond with behavioral changes, creating a moving target that often remains a step ahead of prevention. Almost all causes of death that are on the increase are fueled by high rates of mortality among people with lower education, a trend that counters any progress made in the reduction of today’s health disparities….
Read the entire Eureka News alert
Related articles
- Study takes aim at education-based death rate disparities (eurekalert.org)
- Health gap has grown among young US adults, study finds (eurekalert.org)
- Substantial Health Disparities Among Young US Adults (jflahiff.wordpress.com)
- Call to fight deaths from diabetes (mirror.co.uk)
- New city data to help improve health in neighborhoods (Baltimore Sun)
The State of America’s Children – 2011 Report
![]()
From the Children Defense Fund Web site
CDF’s new report The State of America’s Children 2011 finds children have fallen further behind in many of the leading indicators over the past year as the country slowly climbs out of the recession. This is a comprehensive compilation and analysis of the most recent and reliable national and state-by-state data on population, poverty, family structure, family income, health, nutrition, early childhood development, education, child welfare, juvenile justice, and gun violence. The report provides key child data showing alarming numbers of children at risk: children are the poorest age group with 15.5 million children—one in every five children in America—living in poverty, and more than 60 percent of fourth, eighth and 12th grade public school students are reading or doing math below grade level.
View this year’s interactive report or download the document.
Related articles
- Race and Child Welfare (fosterwee.wordpress.com)
- Op-Ed Columnist: The Decade of Lost Children (nytimes.com)
- Dire State of of America’s Children – by Stephen Lendman (jhaines6.wordpress.com)
- Report: Recession Catastrophic for Children (theroot.com)
- Many child deaths ‘preventable’ (cutie79.wordpress.com)
Health Care Quality Gaps and Disparities Persist in Every State
States are seeing improvements in health care quality, but disparities for their minority and low-income residents persist, according to the 2010 State Snapshots, released today by the Agency for Healthcare Research and Quality (AHRQ).More
Institute of Medicine Report: Better measurement can improve U.S. health outcomes
Institute of Medicine Report: Better measurement can improve U.S. health outcomes
Excerpts from the press release:
Despite medical care expenditures that are the highest of any industrialized nation, deficiencies in the way health information is collected and a lack of agreement on the best indicators by which to measure progress are hindering efforts to improve Americans’ health, according to a new national report.
Released in December by the Institute of Medicine, the report calls on the nation’s health leaders to develop a core, standardized set of indicators to integrate and align health data and health outcome measurement at the national, state and local levels. According to the report, numerous health indicator sets developed in recent years and deployed in different contexts make assessment and comparison difficult for policy-makers and other decision-makers by highlighting similar information in different ways….
The report committee’s vision of the factors that create health in populations — community-based factors and social and environmental determinants — is “very different” from the way the current U.S. health care delivery system is structured, said Gold, noting that the report calls on the U.S. Department of Health and Human Services to produce an annual report informing policy-makers, health leaders and the public about important trends and disparities in the social and environmental determinants that affect health.
“The public health community…shares a commonality of interests and insight as to what the true determinants of health are, and what this report tries to put into sharp relief is that we need to do a better job of measuring the variables that create and detract from health in this country, and that we need to move that measurement strategy away from traditional biomedical variables,” said Gold, who is a professor and chair of community health and social medicine at the Sophie Davis School of Biomedical Education at the City College of New York.
The report, “For the Public’s Health: The Role of Measurement in Action and Accountability,” also recommends that the United States adopt a single, summary measure of population health. Death rates have long been used as the standard measure of population health, the report said, but life expectancy by itself cannot capture information about the health-related quality of life associated with chronic illnesses and injuries. Summary measures of population health, such as health-adjusted life expectancy, capture an overall picture of the well-being of communities.
Moreover, the report recommends that HHS assign the National Center for Health Statistics a leadership role in a “renewed population-health information system” through better coordination and integration of the determinants of health. The report further recommends that the National Prevention, Health Promotion and Public Health Council — the federal body created as part of last year’s health reform law — update Congress annually on NCHS’ progress in assuming such a leadership role.
To ensure the public’s awareness of the quality, safety, efficiency and appropriateness of clinical care services delivered in their communities, the report calls on state and local public health agencies in each state to collaborate with clinical care delivery systems. Local performance reports about overuse, underuse and misuse should be made available for selected interventions, the report said, including preventive and diagnostic tests, procedures and treatment.
The report also recommends that HHS work with relevant federal, state and local public-sector and private-sector partners and stakeholders to develop a performance-measurement system that promotes accountability among governmental and private-sector organizations that have responsibilities for protecting and improving population health at local, state and national levels.
Authoring committee member Martin J. Sepulveda, MD, FACP, called the report a “wake-up call” to the health care delivery system, policy-makers, governmental public health leaders, employers and other payers.
“It tells policy-makers that you can control the ‘mix’ part of total cost by focusing on the medical care delivery system — namely the proportions of controlled versus complicated people with chronic diseases, but the avalanche of new people with chronic diseases will continue to flood the system and will keep total cost high,” Sepulveda, IBM fellow and vice president for integrated health services at IBM Corp. in Somers, N.Y., told The Nation’s Health.
The report also tells governmental public health that it needs to “think differently” about its role in the health crisis and forge new relationships with the health care delivery system to break down barriers and create and use shared pools of data to inform policy-makers and consumers about critical performance matters such as overuse, underuse and misuse of medical care, Sepulveda said.
“It needs to play a key role in helping people know where health care value lies and who is and isn’t delivering it in their communities,” Sepulveda said.
Sponsored by the Robert Wood Johnson Foundation, the report is the first of three on public health strategies to improve health. Reports examining public health and the law and public health and financing are due to be released within the next year.
For more information or to read the report, visit www.iom.edu/reports.
Enabling Personalized Medicine through Health Information Technology: Advancing the Integration of Information
Enabling Personalized Medicine through Health Information Technology: Advancing the Integration of Information

From the Brookings Institute Executive Summary
With federal officials pursuing the goal of a personal human genome map under $1,000 in five years (White House, 2010), it is possible to envision a future where treatments are tailored to individuals’ genetic structures, prescriptions are analyzed in advance for likely effectiveness, and researchers study clinical data in real-time to learn what works. Implementation of these regimens creates a situation where treatments are better targeted, health systems save money by identifying therapies not likely to be effective for particular people, and researchers have a better understanding of comparative effectiveness (President’s Council of Advisors on Science and Technology, 2010).Yet despite these benefits, consumer and system-wide gains remain limited by an outmoded policy regime. Federal regulations were developed years before recent advances in gene sequencing, electronic health records, and information technology. With scientific innovation running far ahead of public policy, physicians, researchers, and patients are not receiving the full advantage of latest developments. Current policies should leverage new advances in genomics and personalized medicine in order to individualize diagnosis and treatment. Similarly, policies creating incentives for the adoption of health information technology should ensure that the invested infrastructure is one that supports new-care paradigms as opposed to automating yesterday’s health care practices.
To determine what needs to be done, a number of key leaders from government, academia, non-profit organizations, and business were interviewed about ways to promote a better use of health information technology to enable personalized medicine. The interviews focused on policy and operational issues surrounding interoperability, standards, data sharing protocols, privacy, predictive modeling, and rapid learning feedback models.
This paper outlines the challenges of enabling personalized medicine, as well as the policy and operational changes that would facilitate connectivity, integration, reimbursement reform, and analysis of information. Our health system requires a seamless and rapid flow of digital information, including genomic, clinical outcome, and claims data. Research derived from clinical care must feed back into assessment in order to advance care quality for consumers. There currently are discrete data on diagnosis, treatment, medical claims, and health outcomes that exist in parts of the system, but it is hard to determine what works and how treatments differ across subgroups. Changes in reimbursement practices would better align incentives with effective health care practices……
A related commentary…
A commentary featured in the January 19 issue of The Journal of the American Medical Association (JAMA) from AHRQ Health IT grant recipient, Alex Krist, M.D. calls for the design of a patient-centered health information system that goes beyond the Personal Health Record. Krist explains that in order for technology to be used, a system should be designed to help patients access health information, interpret data from multiple sources and serve as a tool to facilitate action. Select to access the abstract.
(For suggestions on how to get this article for free or at low cost, click here)
Related articles
March 28, 2011 4:00:00 PM EDT Share
CDC Health Disparities and Inequalities Report – United States – 2011 (And Link About Recent WHO Report on Inequities and Avoidable Deaths)
In my humble opinion, a strong argument for affordable, accessible health care for all regardless of one’s income or where one lives. Health disparities are not found only within groups of people who have the ability to pay for treatments or who are able to get needed treatment quickly.
While this train of thought may be labeled as creeping socialism, health care cost/access challenges are a matter of justice and fairness for all. Is there agreement on what is just or what is fair? Well, no. However, I believe we all can put differences aside in working for what is best for all.
From the Centers for Disease Control and Prevention (CDC) January 13th news release
Americans’ differences in income, race/ethnicity, gender and other social attributes make a difference in how likely they are to be healthy, sick, or die prematurely, according to a report by the Centers for Disease Control and Prevention.
For instance, state-level estimates in 2007 indicate that low income residents report five to 11 fewer healthy days per month than do high income residents, the report says. It also says men are nearly four times more likely than women to commit suicide, that adolescent birth rates for Hispanics and non-Hispanic blacks are three and 2.5 times respectively those of whites, and that the prevalence of binge drinking is higher in people with higher incomes.
The data are in the new “CDC Health Disparities and Inequalities Report — United States, 2011”. The report also underscores the need for more consistent, nationally representative data on disability status and sexual orientation.
“Better information about the health status of different groups is essential to improve health. This first of its kind analysis and reporting of recent trends is designed to spur action and accountability at the federal, tribal, state and local levels to achieve health equity in this country,” said CDC Director Thomas R. Frieden, M.D., M.P.H.
The report, the first of a series of consolidated assessments, highlights health disparities by sex, race and ethnicity, income, education, disability status and other social characteristics. Substantial progress in improving health for most U.S. residents has been made in recent years, yet persistent disparities continue.
Released as a supplement to CDC’s Morbidity and Mortality Weekly Report, the report addresses disparities at the national level in health care access, exposure to environmental hazards, mortality, morbidity, behavioral risk factors, disability status and social determinants of health – the conditions in which people are born, grow, live and work.
Findings from the report’s 22 essays include:
In 2007, non-Hispanic white men (21.5 per 100,000 population) were two to three times more likely to die in motor vehicle crashes than were non-Hispanic white women (8.8 per 100,000). The gender difference was similar in other race/ethnic groups.
In 2007, men (18.4 per 100,000) of all ages and races/ethnicities were approximately four times more likely to die by suicide than females (4.8 per 100,000).
In 2007, rates of drug-induced deaths were highest among non-Hispanic whites (15.1 per 100,000) and lowest among Asian/Pacific Islanders (2.0 per 100,000).
Hypertension is by far most prevalent among non-Hispanic blacks (42 percent vs. 29 percent among whites), while levels of control are lowest for Mexican-Americans (31.8 percent versus 46.5 percent among non-Hispanic whites).
Rates of preventable hospitalizations increase as incomes decrease. Data from the Agency for Healthcare Research and Quality indicate that eliminating these disparities would prevent approximately 1 million hospitalizations and save $6.7 billion in health care costs each year.
Rates of adolescent pregnancy and childbirth have been falling or holding steady for all racial/ethnic minorities in all age groups. However, in 2008, disparities persist as birth rates for Hispanic adolescents (77.4 per 1,000 females) and non-Hispanic black adolescents (62.9 per 1,000 females) were three and 2.5 times those of whites (26.7 per 1,000 females), respectively.
In 2009, the prevalence of binge drinking was higher in groups with incomes of $50,000 or above (18.5 percent) compared to those with incomes of $15,000 or less (12.1 percent); and in college graduates (17.4 percent), compared to those with less than high school education (12.5 percent). However, people who binge drink and have less than $15,000 income binge drink more frequently (4.9 versus 3.6 episodes) and, when they do binge drink, drink more heavily (7.1 versus 6.5 drinks).
The report supports the Healthy People 2020 goals and the forthcoming National Partnership for Action (NPA) to End Health Disparities. The report also complements the upcoming AHRQ National Healthcare Disparities Report *** and underscores the need to connect those working in clinical care and public health, especially at the local level.
“CDC publishes this report today not only to address gaps in health between populations in our country but also to begin to measure progress in years to come in reducing these gaps and inequities going forward,” said Leandris Liburd, Ph.D., M.P.H., M.A., recently appointed director of CDC’s Office of Minority Health and Health Equity. Dr. Liburd will provide leadership for the office and CDC’s public health programs, policies, surveillance and research efforts in achieving health equity.
The full “CDC Health Disparities and Inequalities Report — United States, 2011”, is available at http://www.cdc.gov/mmwr.
*** AHRQ National Healthcare Disparities Report Fact Sheet
AHRQ- Measure Healthcare Quality, including section on National Healthcare Disparities Reports (2003-09) with related documents
Related articles
- Inequities and Avoidable Deaths (thirdworlddd.wordpress.com)
Excerpts- When there are disparities, especially in health, there result avoidable deaths. The WHO estimates that better use of existing preventive measures could reduce the global burden of disease by as much as 70% (WHO, 3). That means that we already have much of the needed solutions, but why are we not implementing them? For example, Diarrheal Disease is a preventable, avoidable disease; with basic sanitation and access to clean water, a huge difference could be made in eradicating the affliction. Why are these things not being put into place?
- What we can take from this is that we need to change the way we look at the disparities, by getting our hands dirty. We need to get into these places and ask questions, not answer them ourselves. The extent of human suffering is vast, but it needs to be witnessed in order to gain solutions. If these people can bare to live their lives full of inequities, inequalities, and misfortune, we can bare to listen to what they have to say.
- Disability as a Disparity (couragecenter.wordpress.com)
About

This blog presents a sampling of health and medical news and resources for all. Selected articles and resources will hopefully be of general interest but will also encourage further reading through posted references and other links. Currently I am focusing on public health, basic and applied research and very broadly on disease and healthy lifestyle topics.
Several times a month I will post items on international and global health issues. My Peace Corps Liberia experience (1980-81) has formed me as a global citizen in many ways and has challenged me to think of health and other topics in a more holistic manner.
Do you have an informational question in the health/medical area?
Email me at jmflahiff@yahoo.com
I will reply within 48 hours.
This blog is a companion site to my Health and Medical News and Resources Web site with…
- Great places to start (locating health information)
- Links to help from others (as health care providers and support groups)
- Interactive tools (as health calculators and apps)
- Select related news sites and blogs
My professional work experience and education includes over 15 years experience as a medical librarian and a Master’s in Library Science. In my most recent position I enjoyed contributing to our library’s blog, performing in depth literature searches, and collaborating with faculty, staff, students, and the general public.
While I will never be be able to keep up with the universe of current health/medical news, I subscribe to the following to glean entries for this blog.
- Science Daily – Your source for the latest research news
- MedlinePlus email updates from the US National Institutes of Health
- Partners in Information Access for the Public Health Workforce – a collaboration of U.S. government agencies, public health organizations and health sciences libraries
- US Agency for Healthcare Research and Quality (AHRQ) news now with updates on the agency’s efforts to “improve the quality, safety, efficiency, and effectiveness of health care for all Americans”
- Research Buzz, “news about search engines, digital archives, online museums, databases, and other Internet information collections since 1998”
- Scout Report, a “weekly publication offering a selection of new and newly discovered Internet resources of interest to researchers and educators”
- KevinMD.com -“Social Media’s leading physician voice”
- EurekAlert-Medicine and Health

{kind=link}